
The Nine Axioms are not a process. They are a filter.
Before I advance a recommendation, I use them to test whether the plan is grounded in how healthcare actually works across patients, workforce, operations, capital, equity, incentives, and the built environment.
A plan does not need to solve every axiom equally. But it should be able to explain how it responds to each one.
Why this matters.
Healthcare plans often fail because they move forward before the hard questions have been answered.
The axioms help pressure-test whether a recommendation is ready for the real world:
Does it improve access, outcomes, or flow?
Can the workforce sustain it?
Does it reflect patient behavior and expectations?
Does the data explain the problem, or only describe it?
Are leaders aligned on the actual tradeoffs?
Will the plan improve outcomes for the people most likely to be left behind?
Used well, the axioms help leaders avoid elegant plans that collapse in execution.
How to read the Axioms
Each axiom is paired with a question I use to test strategy, planning, access, experience, and transformation recommendations before they move forward.
The goal is not philosophical agreement. The goal is readiness: can the recommendation survive the conditions it will actually face?
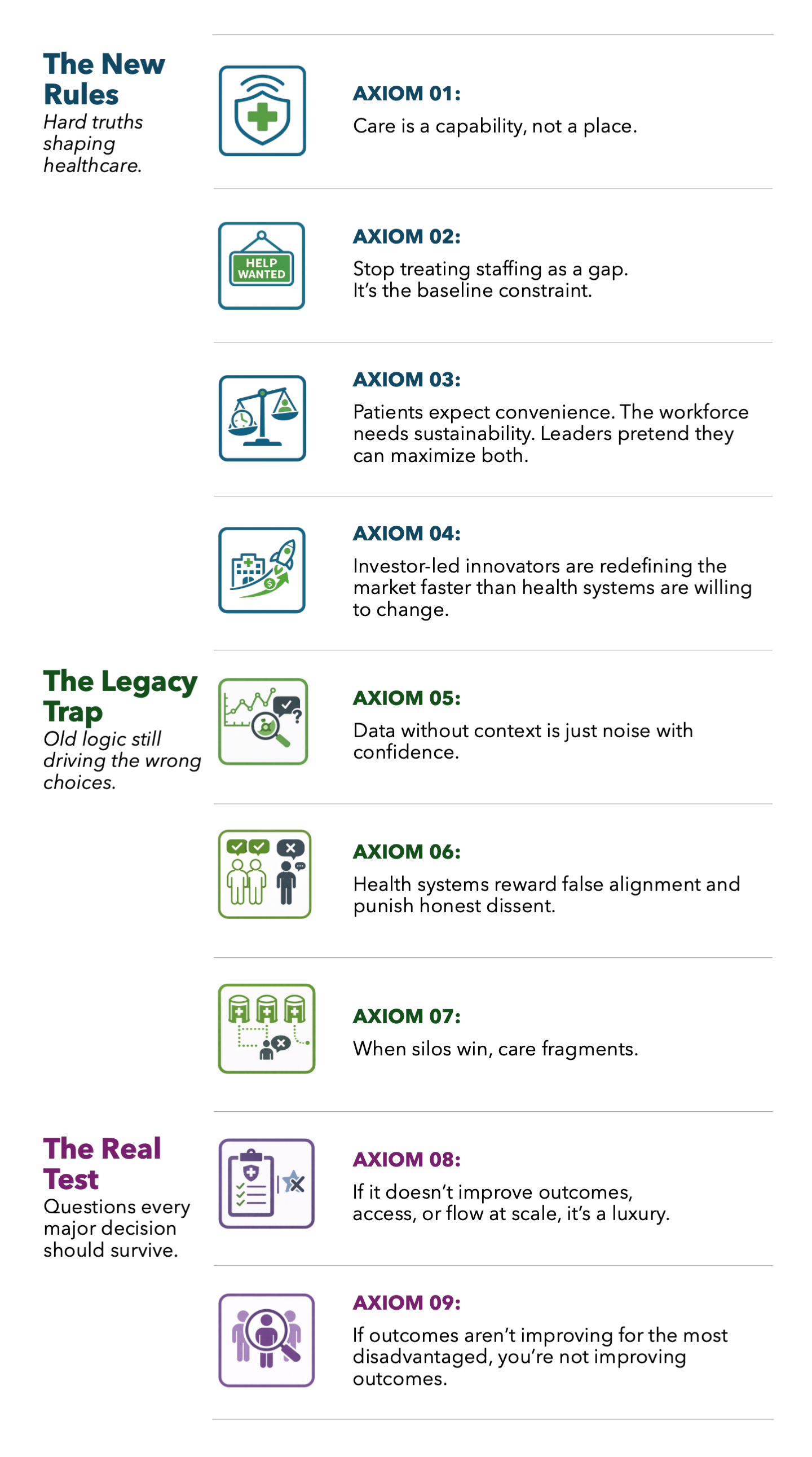
The New Rules
Hard truths shaping healthcare.

AXIOM 01: Care is a capability, not a place.
Care needs should define the setting, not habit, footprint, or bed count.
QUESTION: What capability does this patient actually need, and what setting is truly required to deliver it safely?

AXIOM 02: Stop treating staffing as a gap. It’s the baseline constraint.
Too many plans assume labor the organization does not have and is unlikely to get.
QUESTION: Why are we expanding a care model we cannot reliably staff today?

AXIOM 03: Patients expect convenience. The workforce needs sustainability. Leaders pretend they can maximize both.
Healthcare keeps making service promises the labor model cannot safely sustain. QUESTION: What convenience are we promising that the workforce cannot keep delivering safely and reliably?

AXIOM 04: Investor-led innovators are redefining the market faster than health systems are willing to change.
Narrower, faster models are taking profitable share while incumbents defend legacy scope.
QUESTION: Where are innovators exposing parts of our model that are too broad, too slow, or too expensive to compete?
The Legacy Trap
Old logic still driving the wrong choices.

AXIOM 05: Data without context is just noise with confidence.
A metric can look precise while pointing leaders toward the wrong fix.
QUESTION: What is actually driving the numbers, and what are we misreading if we mistake the metrics for the problem?

AXIOM 06: Health systems reward false alignment and punish honest dissent.
Political comfort often wins over truth, speed, and better decisions.
QUESTION: Are we resolving disagreement on the merits, or punishing the people willing to surface inconvenient truths?

AXIOM 07: When silos win, care fragments.
The patient journey breaks when departments optimize for themselves and no one owns what happens next.
QUESTION: Who owns the journey end to end, and what in our structure or incentives makes that harder than it should be?
The Real Test
Questions every major decision should survive.

AXIOM 08: If it doesn’t improve outcomes, access, or flow at scale, it’s a luxury.
Health systems overfund what is attractive and underfund what actually moves performance.
QUESTION: What are we not funding, improving, or fixing if we choose this instead?

AXIOM 09: If outcomes aren’t improving for the most disadvantaged, you’re not improving outcomes.
Averages can improve while disparities remain untouched.
QUESTION: Who is still not improving, and what are our averages hiding?

How These Axioms Shape My Work
I use these axioms before advancing recommendations.
They help test whether a plan is grounded in operational reality, responsive to patient and workforce needs, clear about tradeoffs, attentive to equity, and durable enough to survive implementation.
Every recommendation should be able to explain how it responds to the relevant axioms.
If it cannot, it is not ready.