
Regionalizing Care to Relieve Pressure on a Legacy Regional Teaching Hospital
The ask
A large, multi-campus health system needed a campus master plan to address aging facilities, capacity constraints, and future growth. The unstated expectation was to determine where, and how the organization should invest limited capital over time.
The problem wasn’t the campus.
It was the system.
The organization was operating as a collection of sites making independent decisions, without a shared definition of success or a clear view of how care should be delivered across the region. Leadership lacked alignment on what “winning” meant, with priorities ranging from growth to experience to academic ambition—often in conflict.
At the same time:
Core facilities were aging, undersized, and increasingly misaligned with modern care delivery
Infrastructure deterioration was creating operational and safety risk
Market share was under pressure across key service lines
A highly vulnerable patient population was driving demand into the most resource-intensive settings
The organization continued to think like an academic medical center despite functioning as a regional teaching system
The organization was trying to solve for buildings, without first aligning on what kind of system it needed to be.
What was really going on
Where the tension was
Several forces were pulling the organization in different directions:
Strategic identity vs. aspiration
Academic ambition vs. the realities of a regional care delivery system
Capital ambition vs. market reality
Strong internal advocacy for major investments that were not clearly supported by demand
System thinking vs. site-based decision-making
Individual campuses optimizing locally, without a coherent enterprise strategy
Urgency vs. alignment
Pressure to act quickly in the face of aging infrastructure, without agreement on what success looked like
Stability vs. disruption
A major competitive move mid-process introduced new uncertainty into an already complex planning environment
What changed the trajectory
The work did not start with buildings.
It started with forcing clarity on the decisions that drive them.
Three shifts changed the trajectory:
Defining the system first
Aligning leadership on what the organization is—and is not—so that strategy, operations, and capital decisions could follow
Making tradeoffs explicit
Moving from competing definitions of success to a shared understanding of what matters most—and what does not
Designing care delivery before designing space
Defining how care should function across the region, then translating that into volumes, programs, and ultimately facilities
This created a plan that could absorb disruption, including competitive changes, without needing to be reworked midstream.
What changed in the end
The result was not a traditional master plan.
It was a set of decisions that repositioned the system:
From sites to system
A shift toward a coordinated, regional care delivery model with clearly defined roles for each campus
From broad ambition to targeted growth
Focused investment in areas of real opportunity, while avoiding misaligned capital decisions
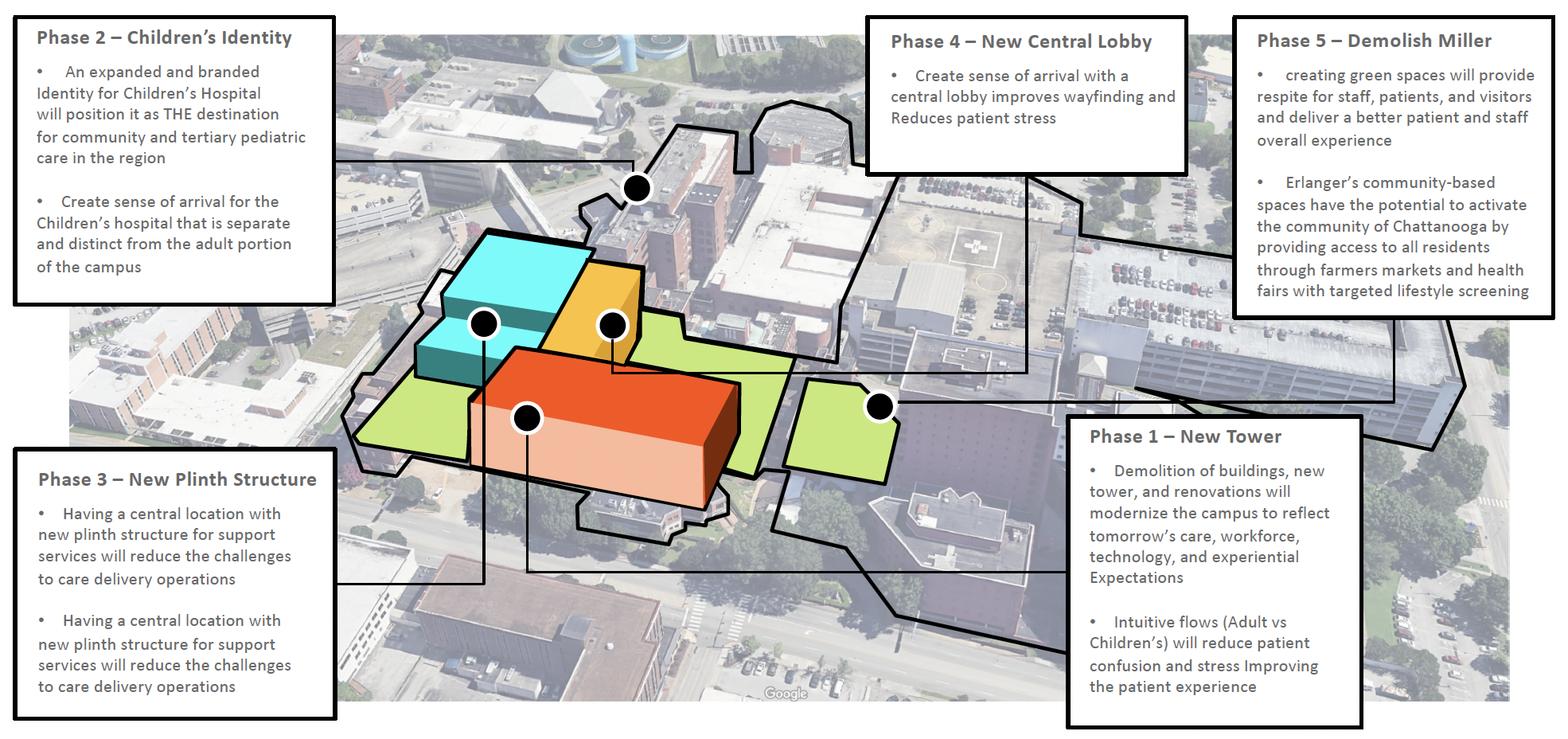
From reactive capital to phased modernization
A roadmap to address aging infrastructure without disrupting ongoing operations or care delivery
What this case reveals
Campus planning fails when it starts with buildings.
It works when it starts with clarity.
The built environment is not the strategy, it is the consequence of it.
When leaders align on what they are solving for, capital becomes more disciplined, decisions become clearer, and the plan holds, even as conditions change.