
Designing Emergency Care for Extreme Volume, High Acuity, and Cultural Complexity
The ask
A flagship academic medical center in Qatar needed a new emergency department and trauma center designed in time for the 2022 FIFA World Cup and planned annual volumes exceeding 520,000 patients. The facility had to accommodate extraordinary volume, multiple arrival modes, and local cultural expectations without breaking under real-world volume, acuity, and operational complexity.
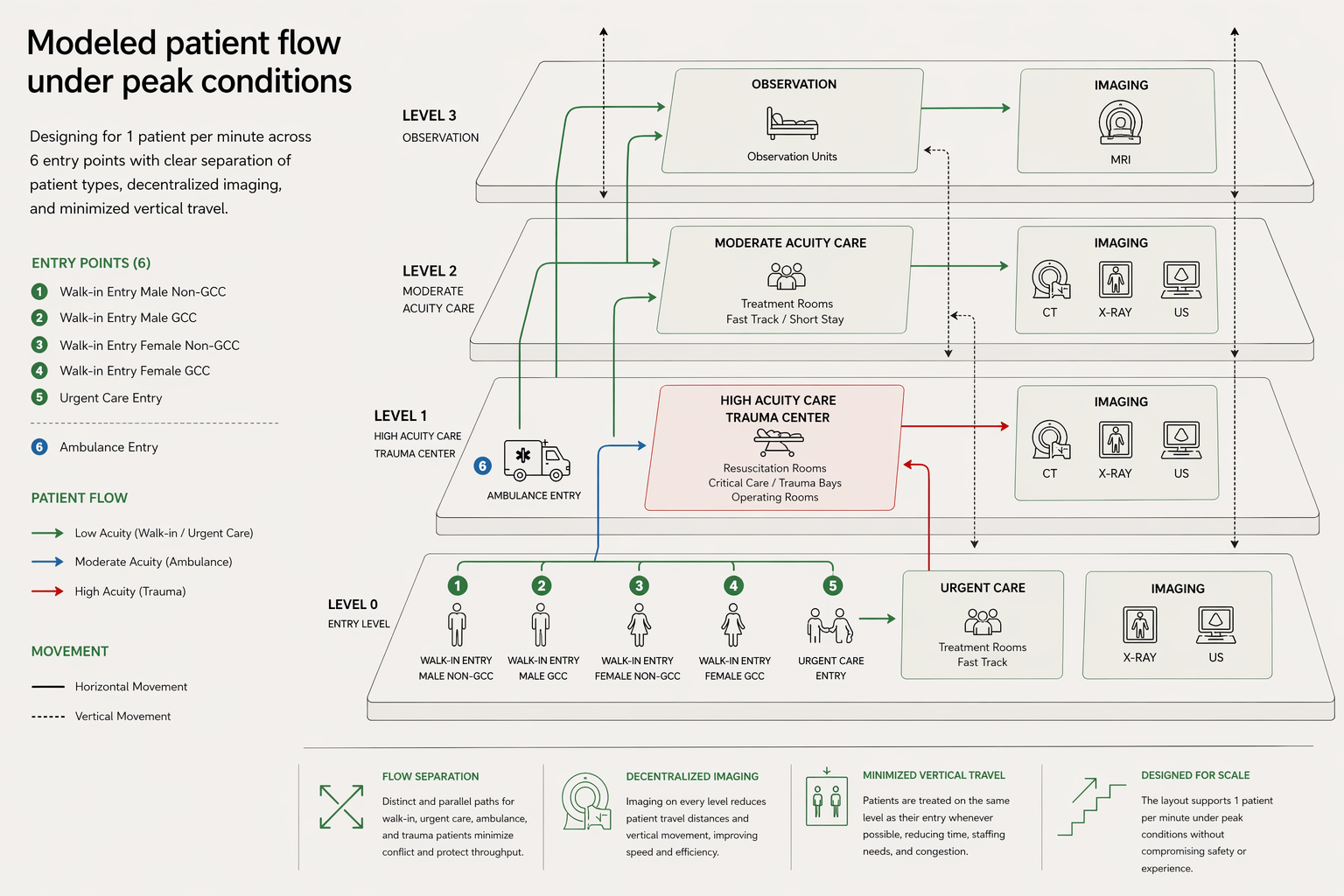
This was not just an emergency department design project. It was a large-scale operating model problem disguised as architecture. The system needed to manage one patient arrival per minute across six different entry points, while supporting radically different levels of acuity, from low-complexity walk-ins to trauma resuscitations. The real challenge was not where to put rooms. It was how to create an emergency and trauma environment whose circulation logic would allow the entire system to function under pressure.
What was really going on
Where the tension was
Emergency medicine, trauma, and radiology were each focused on the needs of their own patient populations, but not yet aligned around what the department as a whole needed to do. The team was trying to optimize individual components of the system while designing one of the busiest emergency environments in the world. What was needed was not local optimization. It was system-level flow. Radiology favored centralized imaging, a clinically logical choice that would have broken the system at scale. It would have required many patients to move vertically through the multi-story building, increasing travel time, staffing burden, and the risk of throughput breakdowns.
What changed the trajectory
I shifted the work from department-by-department preference setting to performance-based operating model design.
We analyzed tens of thousands of throughput data points and built a discrete-event simulation model to test how different flows would perform under real conditions: travel distances, vertical movement, conflicting paths, and separation of front- and back-of-house circulation.
That changed the conversation.
Instead of debating opinions, the team could see the operational consequences of each design decision. The work moved from designing a building to engineering how the system would behave under stress.
From there, we used decision accelerator sessions to force tradeoffs, align stakeholders around the best-performing options, and reconcile the architecture to the operating model the system actually required.
What changed in the end
The final design fundamentally changed how patients, staff, and resources moved through the system.
Decentralized imaging
Imaging was decentralized, reducing patient travel distances by up to 80%, cutting vertical movement nearly in half, and lowering the need for transport resources.
Vertical circulation
Elevator towers were redistributed, reducing travel distance to vertical circulation by roughly one-third.
Flow separation
A multi-level entry strategy separated walk-in, ambulance, and high-acuity traffic while maintaining proximity to the clinical spaces each required.
System outcome
The result was not just a better building. It was a safer, faster, more coherent emergency care system embedded in architecture.
What this case reveals
In high-volume emergency care, architecture is not a backdrop. It is an operating decision.
At scale, small inefficiencies in circulation become structural threats to safety, experience, and throughput. What looks like a design preference becomes a system constraint.
Clinical departments will optimize for themselves unless someone forces the system to be designed around the whole. In complex environments, that whole has to be modeled, tested, and made visible.
Systems at this scale do not fail under ideal conditions. They fail at the margins—during surges, handoffs, and constraints. If those conditions are not designed for explicitly, they become the system.
And in the end, the best emergency environments are not the ones with the most impressive plans. They are the ones whose flow logic survives real volume, real acuity, and real-world use.