
Expanding cancer services in a resource-constrained rural system
The ask
A critical access hospital wanted to create local cancer infusion capacity so patients would no longer have to travel over to 90 minutes for treatment. The challenge was doing so on an aging campus with limited capital and little room for error.
The infusion center was the visible need, but the real issue was that the hospital did not have the space, infrastructure, or operating flexibility to add it cleanly. Making the project work meant confronting the fact that the existing configuration of services, staffing, and space could not simply absorb a new strategic priority.
What was really going on
Where the tension was
Every viable solution triggered consequences somewhere else. Creating space for infusion required addressing pharmacy capacity, ICU location, inpatient staffing, and clinical adjacencies. The proposed relocation of the ICU to co-locate with the medical-surgical unit created concern among nursing staff, and the age of the building meant every renovation risked exposing additional problems. The organization could not afford the wrong move, but the right move required putting long-standing assumptions back on the table.
What changed the trajectory
I reframed the project from “where do we put the infusion center?” to “what has to change across the hospital to make this possible?” That shifted the work from space planning to system re-sequencing. Instead of evaluating options in isolation, we mapped the second- and third-order implications of each decision across operations, staffing, and capital. That made it possible to align leadership around a phased plan that treated the infusion center not as an addition to the existing model, but as a strategic move that required the rest of the hospital to adapt.
What changed in the end
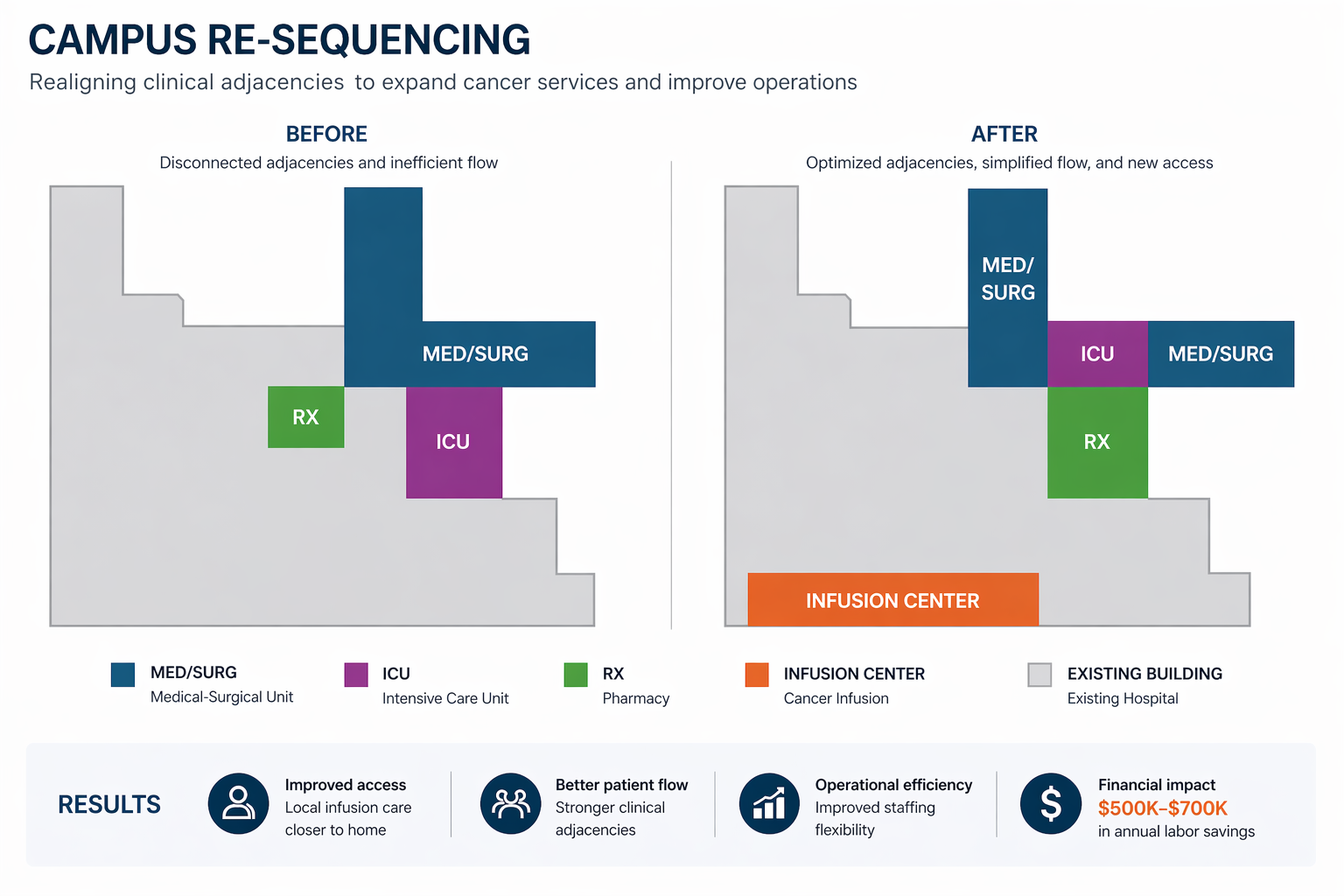
The hospital was able to move forward with a new cancer infusion center while reconfiguring adjacent services to support it.
Operational reconfiguration
Pharmacy capacity was addressed, the ICU was relocated to co-locate with the medical-surgical unit, and inpatient staffing flexibility improved.
Access impact
Local patients no longer needed to travel up to 90 minutes for infusion care.
Financial impact
The reconfiguration generated approximately $500,000–$700,000 in annual labor savings, offsetting a meaningful portion of project cost.
What this case reveals
In resource-constrained systems, the right strategic decision is often not the hard part. The hard part is being willing to reconfigure everything that decision makes newly impossible.
Adding a new capability is rarely additive. In constrained environments, every strategic move creates second- and third-order consequences across space, staffing, operations, and capital.
In these settings, nothing gets grandfathered in. Legacy footprint, legacy workflows, and legacy staffing models all have to be put back on the table.
And in the end, the most dangerous mistake is not making the wrong strategic choice. It is making the right one while refusing to accept the structural changes it requires.